
In emergency rooms, triage identifies immediate-risk patients well, but reduces strong clinical heterogeneity in a few classes of urgency. Within the same class, very different patients (by acute physiological severity or clinical/management complexity) are often managed as if they were operationally equivalent.
This poor structuring of intra-class priority results in:
- high decision-making discretion
- variability between operators
- Inefficiencies in flows especially in congested conditions and increased waiting times for the most vulnerable patients
In addition, much relevant information is contained in unstructured texts (brief history, nursing notes) and is difficult to use with traditional tools. Thus, decision support is needed that structures and enhances the information already available at triage, improving operational decisions without replacing clinical judgment. The implementation was developed in a medium to large emergency department with daily accesses close to 150 patients.
Methodological approach
Step 1: LLM “domain-adapted” pipeline with clinical validation
- Integration of structured data (vital parameters, age, gender) and triage texts.
- Normalization of clinical text (corrections, acronym expansion, semantic standardization).
- LLM inference calibrated with prompts designed and validated with PS physicians.
- Output: two ordinal assessments per patient:
- Intensity (acute physiological severity)
- Complexity (vulnerability and management burden
If triage remains unchanged: the model adds a second level of decision-making.
Step 2: “Agentic” prioritization algorithm + operational simulation
- LLM measures feed into an algorithm that proposes intra-class prioritization via composite index (weighting between intensity and complexity).
- Evaluation by discrete-event simulation, isolating the effect of the prioritization rule alone at constant demand/capacity.
- The system acts as real-time decision support: it produces interpretable operational signals and improves performance without changing clinical protocols.
Results
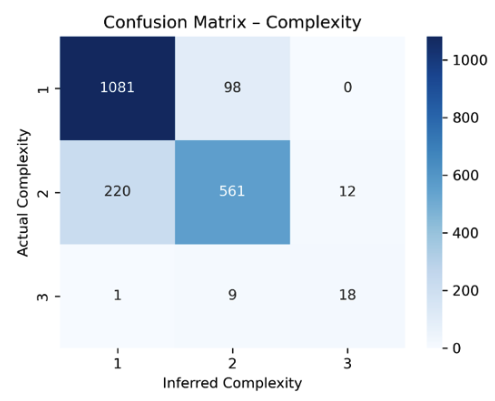
Alignment with clinical judgment
The model’s assessments are consistent with independent medical assessments, particularly on the complexity dimension.
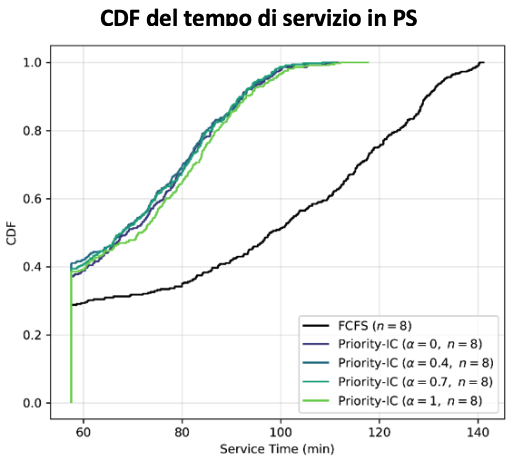
Reduced waiting time in congestion
Secondary prioritization based on intensity+complexity reduces the average waiting time in the analyzed class by about 19-29 minutes per patient, with indirect benefits on other classes as well.
Improving overall flow
A more structured redistribution of waits reduces systemic congestion by targeting the most delay-sensitive patients and limiting service time inflation.
More transparent and governable decisions
Makes explicit what are now informal logics, improving transparency, reproducibility and governance of the process.



